Sustained fat loss comes down to one fundamental principle: you must consistently consume less energy than you
expend. A sustained caloric deficit is required for ongoing fat loss.
It doesn't matter how you achieve that deficit (for example, following a lifestyle meal plan (keto, paleo, or low carb)
or simply just eating less) - what matters is that you are consistent in maintaining that deficit. Use any protocol
that will make it easier for you maintain that consistency.
It's important to note that losing weight is not the same as losing fat. The goal for most people is to reduce fat mass
while preserving as much lean mass as possible. Doing that requires managing the deficit intelligently, alongside ensuring
adequate protein intake, sleep, and hydration. Resistance training plays a central role in this process - improving body
composition and physical function.
The TL;DR
Fat loss requires a sustained calorie deficit. Start with 500 calories per
day below your maintenance requirement. (See TDEE and how to estimate it). This is a safe starting
point. You can get much more aggressive with your deficit - but you must maintain adequate protein intake to minimise
muscle catabolism.
Lift weights. Include resistance training 3-5x/week during fat loss to preserve muscle mass and strength. It
counters the muscle catabolism from calorie deficits, improving body composition (more fat loss, less lean muscle loss) alongside
high protein intake. Evidence shows lifters retain significantly more
lean mass in caloric deficits.
Protein matters. Aim for a minimum of 1.5 to 2 grams of protein per kg of body weight per day. Go higher
if you are lean, resistance training, very active or pursuing an aggressive calorie deficit.
Pick a meal plan you can stick to. Low carb, keto, paleo, intermittent fasting, continuous calorie restriction... Anything.
All approaches work if they create a deficit and you can consistently maintain that deficit.
If you don't measure it, you can't manage it. Use scales and an app to log food intake and body weight regularly.
Accuracy and consistency beat guesswork.
Sleep is when the magic happens. Target 7 to 9 hours per night to support fat
loss and muscle retention. This is non-negotiable.
Stay hydrated. Aim for roughly 3 litres of water per day, including water
with meals. Adjust for body size, climate, and activity.
Adjust based on results. If you are not losing 0.5 to 1 percent of body weight
per week after two weeks, reduce your caloric intake by 100 to 200 calories.
Energy Balance
The human body obeys the laws of thermodynamics. When energy intake is chronically lower than energy
expenditure, stored energy must be mobilised. In other words, if you consistently eat less than you expend
then, over time, your body will burn fat (and a little bit of muscle) for energy.
Multiple analyses confirm that weight loss requires a negative energy balance, regardless of dietary pattern.
When calorie intake is matched, different diets produce similar weight loss outcomes.[6,10]
A 2007 paper summarised this bluntly: "independently of the method for weight loss, the negative energy balance
alone is responsible for weight reduction."[1] Whether you
fast, count macros, or follow another structured approach, if you are not in a sustained deficit, you will not
achieve sustained fat loss.
What Is TDEE and How to Estimate It
To create a calorie deficit, you first need a reasonable estimate of how many calories you burn per day. That
estimate is your TDEE (Total Daily Energy Expenditure).
What TDEE means
TDEE is the total energy your body uses in a day. It is made up of:
BMR (Basal Metabolic Rate): energy used at rest to keep you alive.
NEAT (Non-Exercise Activity Thermogenesis): day-to-day movement outside formal exercise, including work,
walking, standing, and general activity.
EAT (Exercise Activity Thermogenesis): planned training such as the gym, running, sport, or
cycling.
TEF (Thermic Effect of Food): energy used to digest and process food.
Most people underestimate or overestimate TDEE because they focus on exercise and ignore NEAT.
For many adults, NEAT is the biggest swing factor between “sedentary” and “very active”.
How to calculate an initial TDEE estimate
In practice, the simplest approach is to estimate your BMR first, then adjust it based on how you actually
live and move day to day.
Treat the output as a starting range, not a perfect number.
Step 1: Estimate BMR (Mifflin–St Jeor)
Use your sex, age, height, and weight to estimate BMR:
Men:BMR = (10 × weight in kg) + (6.25 × height in cm) − (5 × age) + 5
Women:BMR = (10 × weight in kg) + (6.25 × height in cm) − (5 × age) − 161
Step 2: Adjust for your actual activity
Many online calculators ask you to pick an activity level. The problem is that labels like “moderately active"
often reflect exercise sessions, not total daily movement. A better approach is to anchor
your estimate
to step count and occupation.
Use these step-count bands as a rough guide, then adjust based on how physical your work is:
Under 5,000 steps per day: generally sedentary.
5,000 to 8,000: lightly active.
8,000 to 12,000: moderately active.
12,000 to 18,000: very active.
20,000 or more: extremely active.
If you use an activity multiplier, choose it based on the above reality check:
1.2 to 1.3 (sedentary), 1.35 to 1.5 (light), 1.55 to 1.7
(moderate),
1.75 to 1.9 (very active to extremely active). Treat this as an estimate, not a promise.
Examples
Example A: High-movement job (lawnmowing business)
A person running a lawnmowing business may average around 25,000 to 30,000 steps per day,
plus frequent
lifting, carrying, pushing, and bending. Even without formal exercise, their total daily movement is high.
A plausible starting multiplier is often toward the 1.75 to 1.9 range, depending on body
size and workload.
Example B: Low-movement desk job (IT working from home)
An IT worker at a home office might average 2,000 steps per day and sit for long periods.
Even with
three to four gym sessions per week, their overall daily movement can still be low compared with manual
labour.
A plausible starting multiplier is often closer to 1.3 to 1.45, depending on training
volume and lifestyle.
Validate and refine your TDEE
TDEE is not fixed. It changes with body weight, training volume, sleep, stress, and diet-induced shifts in
daily movement.
The most reliable way to refine your estimate is to test it against real data.
Track calorie intake as accurately as you can for 14 to 21 days.
Include oils, sauces, drinks, and snacks.
Weigh daily under consistent conditions (morning, after the bathroom), then focus on the trend
(for example a 7-day average), not single days.
If your trend weight is stable, your average intake is close to your TDEE.
If weight is falling, you are in a deficit. If rising, you are in a surplus.
Once you have a reasonable TDEE estimate, you can set a deficit (for example 500 calories per day) and
adjust
based on outcomes.
For more detail on building a tracking habit that is sustainable, see the tracking
section.
The Deficit Size Matters
How aggressive should the deficit be? The evidence consistently favours moderation. Think of this as a marathon, not a sprint.
You're shooting for life-long change. Start small and adjust the deficit over time as your body adapts.
If you have not estimated your maintenance calories yet, start with the TDEE section and
come back here once you have a reasonable starting point.
A 2021 meta-analysis found that energy deficiency impairs gains in lean mass during resistance training, even
though strength can still improve.[3] In practical terms,
as deficits grow larger, it becomes progressively harder to gain or preserve lean tissue during training.
Very low-calorie diets under 800 kcal per day do produce rapid weight loss, but at a cost. A 2024 systematic
review reported that approximately 25 to 27 percent of total weight lost under these protocols comes
from muscle mass, even when protein intake is adequate.[5] Outcomes vary by population and training status, but the trade-off is clear.
For most people aiming to lose fat while preserving lean mass, a moderate deficit of roughly 500
calories per day provides the best balance between effectiveness and muscle retention.[3,4,6]
Protein: Your Muscle Insurance Policy
Protein intake during weight loss is not optional if lean mass preservation matters.
The evidence shows:
During energy restriction, protein intakes of 1.2 to 1.6 g per kg of body weight per day
preserve lean mass better than standard recommendations[12]
Resistance-trained, very lean, or highly active individuals may benefit from higher intakes, up to
1.6 to 2.4 g/kg/day, particularly during aggressive cuts[15]
A 2024 meta-analysis found that protein intake above approximately 1.3 g/kg/day during
weight loss was associated with better muscle mass preservation, while intake below 1.0
g/kg/day carried higher risk of muscle loss[11]
Protein supports muscle retention through several mechanisms. It is more satiating than carbohydrate or fat,
helping with adherence to the deficit. It has a higher thermic effect, modestly increasing energy expenditure.
Most importantly, it supplies the amino acids required to maintain muscle protein synthesis during periods of
energy restriction, especially when combined with resistance training.[13,14,17]
Sleep: The Overlooked Variable
Sleep has a measurable impact on body composition during weight loss. It is truly when the magic happens.
In a controlled trial, participants undergoing the same calorie restriction lost significantly less fat when
sleeping 5.5 hours per night compared with 8.5 hours, despite identical energy intake.[21] Short sleep shifted weight loss away from fat and
toward lean tissue.
The mechanisms are well documented:
Sleep restriction disrupts appetite regulation and increases energy intake, although individual hormone
responses vary[18,20]
Insufficient sleep impairs glucose metabolism and insulin sensitivity[23]
Poor sleep increases consumption of energy-dense foods[18,25]
A 2023 longitudinal study found that insufficient sleep predicted poorer weight loss maintenance after one
year, independent of other behavioural factors.[19] For
fat loss and maintenance, prioritising 7 to 9 hours of quality sleep is not optional.[24,26]
Hydration: Simple but Supportive
Adequate hydration supports weight loss primarily by improving appetite control, dietary adherence, and
metabolic function.
Evidence indicates:
Drinking approximately 500 ml of water before meals can reduce perceived hunger and energy
intake, particularly in middle-aged and older adults[28,33]
A 12-week intervention found that participants who drank water before meals lost around 2 kg
more than those who did not, under otherwise similar conditions[28]
Adequate hydration supports normal metabolic processes and exercise performance, which indirectly supports
fat loss adherence[27,31]
The adequate intake recommendations for total water are approximately 2.7 litres per day for
women and 3.7 litres per day for men, including water from food sources.[32,34] You do not need to overcomplicate this. Drink when thirsty, include water with meals,
and aim for pale yellow urine.
Adherence: The Real Game
No protocol works if you cannot stick to it. Adherence explains far more of weight loss success than diet
style.
Available Protocols
In real life, people tend to create a calorie deficit in a few common ways:
Continuous Energy Restriction (CER)
Daily calorie reduction of roughly 20 to 30 percent from maintenance.[8]
Intermittent Fasting Variants
Time-Restricted Eating (TRE): Eating within a daily window of 6 to 10 hours[8]
Alternate Day Fasting (ADF): Alternating normal intake days with days at roughly 20 to 30 percent
of normal intake[8]
5:2 Method: Five days of normal eating, two non-consecutive low-calorie days[9]
A 2024 network meta-analysis of 47 randomised controlled trials found that all major caloric restriction
strategies produced weight loss. ADF showed slightly greater short-term loss, but differences were small and not clinically meaningful long term.[8]
Another 2024 meta-analysis comparing fasting-based strategies with continuous restriction found similar
weight loss at six months, with fasting showing a modest short-term advantage that did not persist.[9]
In practice, the best diet is the one you can follow consistently.[6,9]
Finding Your Protocol
Only you know what will work for you... and if you are unsure, remember this is a marathon not a sprint - try different protocols
out and see what feels maintainable for you. Choose based on:
Your daily schedule and lifestyle
Your preference for structure versus flexibility
Your prior successes and failures
Your individual training demands
The physiology is secondary to adherence.
The Partner Effect
Aligning the eating patterns within your household will reduce friction and increase your chances for long-term compliance.
While it might seem easier if you and your partner follow the same protocol, you don't have to. Protocols do not
need to be identical, but they should be compatible.
Track Everything: Measurement Drives Results
Self-reported intake is notoriously unreliable. Don't guess - you will get it wrong.[35] People who consistently track what they eat tend to lose more weight and keep it off for longer:
Greater adherence to food tracking predicts greater weight loss and maintenance[36,37]
Higher frequency of tracking is associated with better results, regardless of method[41,42,43]
Systematic reviews confirm that consistent self-monitoring improves outcomes across behavioural
interventions[41,45]
What to track:
Food intake: including oils, sauces, drinks, and incidental bites[35,45]
Body weight: at least weekly, ideally daily under consistent conditions[38]
The tracking method matters far less than consistency.[40,43,45] However, there are tools that make the process much easier and, therefore,
increase your chances of sticking with it.
If daily weigh-ins feel noisy or discouraging, jump to why the scales lie to
see how to interpret trends properly.
Why the Scales Lie (and How to Read Them Properly)
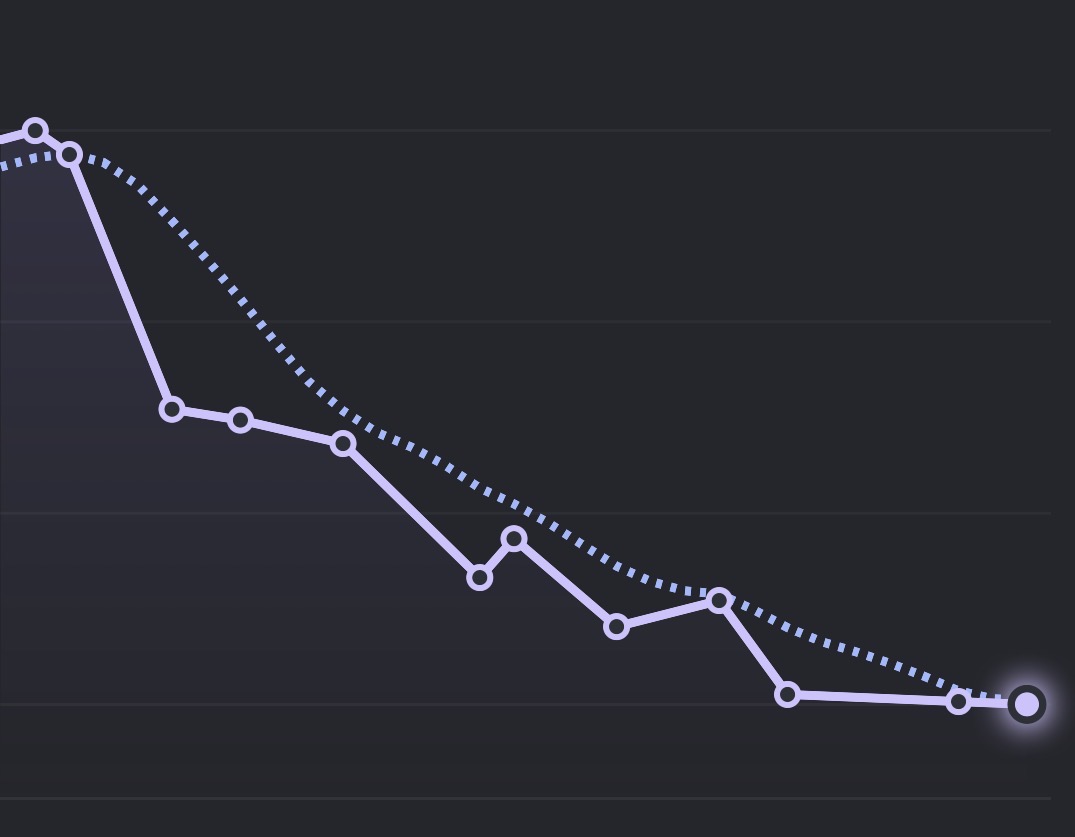
Body weight does not change in a straight line, even when fat loss is occurring. Tracked on a graph, it will look like
a staircase - with periods of plataeu and even little steps up before bigger steps down. Remember, the scale measures
total body mass, not body fat, and short-term fluctuations are dominated by factors that have nothing to do with fat gain or loss.
This is why tracking a trend (the dotted line in the image below) is more important than individual weigh-in results (the solid line).
Don't let increases on the scale mess with your motivation. Increases and plateaus are normal and should be expected.
Stay strong and persist.
Body weight does not change in a straight line, even when fat loss is occurring.
What drives short-term scale changes
Water retention: Changes in sodium intake, carbohydrate intake, inflammation, stress, or hormonal
cycles can shift body water by 1 to 2 kg within days.
Glycogen storage: Stored carbohydrate binds several times its weight in water. Increasing or
reducing carbohydrate intake can move the scale quickly without any fat change.
Gut contents: Fibre intake, meal timing, and digestion alter how much material is physically
present in the gastrointestinal tract.
Training effects: Resistance training causes temporary inflammation and water retention in muscle
tissue, which can mask fat loss on the scale.
Because fat loss occurs slowly, often at 0.5 to 1 percent of body weight per week,
these faster moving variables can completely obscure real progress when weight is
assessed over short time frames.
Why the scale can stall during body recomposition: If you are strength training while eating in a
calorie deficit,
it is possible to lose fat and gain some muscle at the same time, especially if you are new to lifting or
returning after a break.
For example, losing 5 kg of fat while gaining 1 kg of muscle would show only a 4 kg change on the scale,
even though your body
looks leaner, clothes fit better, and strength improves.
This is not failure. It is body recomposition.
In this situation, the scale alone becomes a poor progress marker.
Waist measurements, progress photos, how clothes fit, and strength trends often tell a more accurate story.
How to use the scale correctly
Weigh under consistent conditions, ideally daily, first thing in the morning
after using the bathroom.
Focus on trends, not single measurements. A rolling 7-day average is
far more informative than day-to-day changes.
Judge progress over weeks, not days. Two to three weeks of data is the minimum
needed to assess whether a calorie target is working.
When interpreted properly, the scale is a useful tool. When interpreted in isolation
or over short periods, it can be actively misleading. Fat loss is a slow biological
process layered under fast, noisy fluctuations in body weight.
This is why resistance training is foundational during fat loss. It protects lean mass, improves how your
body uses energy, and often explains why the scale stalls even as health, strength, and appearance improve. Read more in Strength Training for Longevity.
Hot tip: Track waist circumference alongside scale weight.
Measure around the waist at the level of the navel, under the same conditions each time,
ideally once per week. Waist measurements often reflect fat loss even when scale weight
temporarily increases due to water retention. Seeing your waistline trend down while
weight fluctuates can reduce frustration and help you stay consistent.
Putting It Together
Establish a moderate deficit: approximately 500 calories per day below maintenance[3,6]
Set protein intake: 1.2 to 1.6 g/kg body weight, higher if lean or highly active[11,12,15]
Adjust as needed: If weight loss is below 0.5 to 1 percent of body weight per week after two weeks, reduce
intake by 100 to 200 calories See plateaus.
There are no magic foods, metabolic hacks, or shortcuts. The fundamentals are energy deficit, sufficient
protein, sleep, hydration, and consistency. That is the game.
Strasser B, Spreitzer A, Haber P. Fat loss depends on energy deficit only, independently of the
method for weight loss. Ann Nutr Metab. 2007;51(5):428 to 32. doi: 10.1159/000111162. Available at: PubMed
Hector AJ, McGlory C, Damas F, et al. Pronounced energy restriction with elevated protein intake
results in no change in proteolysis and reductions in skeletal muscle protein synthesis that are mitigated by
resistance exercise. FASEB J. 2018;32(1):265 to 275. doi: 10.1096/fj.201700158RR. Available at: PubMed
Murphy CH, Hector AJ, Phillips SM. Energy deficiency impairs resistance training gains in lean
mass but not strength: A meta-analysis and meta-regression. Scand J Med Sci Sports. 2021;31(Suppl
1):125 to 137. doi: 10.1111/sms.14075. Available at: PubMed
Koliaki C, Spinos T, Spinou M, Brinia ME, Mitsopoulou D, Katsilambros N. Defining the Optimal
Dietary Approach for Safe, Effective and Sustainable Weight Loss in Overweight and Obese Adults.
Healthcare (Basel). 2018;6(3):73. doi: 10.3390/healthcare6030073. Available at: MDPI
Barreira JV, Bandeira PFR, do Nascimento Marreiro D. A Systematic Review and Meta-Analysis of the
Effect of Caloric Restriction on Skeletal Muscle Mass in Individuals with, and without, Type 2 Diabetes.
Nutrients. 2024;16(19):3328. doi: 10.3390/nu16193328.
Available at: MDPI
Kim JY. Optimal Diet Strategies for Weight Loss and Weight Loss Maintenance. J Obes Metab
Syndr. 2021;30(1):20 to 31. doi: 10.7570/jomes20065.
Available at: PubMed
Reilly EE, et al. A Systematic Review of Dietary Supplements and Alternative Therapies for Weight
Loss. Obesity (Silver Spring). 2021;29:1102 to 1113. doi: 10.1002/oby.23110. Available at: Wiley
Liu D, Huang Y, Huang C, et al. Comparing caloric restriction regimens for effective weight
management in adults: a systematic review and network meta-analysis. Int J Behav Nutr Phys Act.
2024;21:108. doi: 10.1186/s12966
to 024-01657 to 9. Available at: BMC
Cioffi I, Evangelista A, Ponzo V, et al. Is Fasting Superior to Continuous Caloric Restriction
for Weight Loss and Metabolic Outcomes in Obese Adults? A Systematic Review and Meta-Analysis of Randomized
Clinical Trials. Nutrients. 2024;16(20):3533. doi: 10.3390/nu16203533.
Available at: MDPI
Hall KD, Heymsfield SB, Kemnitz JW, Klein S, Schoeller DA, Speakman JR. Energy balance and its
components: implications for body weight regulation. Am J Clin Nutr. 2012;95(4):989 to 994. doi: 10.3945/ajcn.112.036350.
Chung N, Park MY, Kim J, et al. Enhanced protein intake on maintaining muscle mass, strength,
and physical function in adults with overweight/obesity: A systematic review and meta-analysis. Clin
Nutr. 2024;43(7):1737 to 1750. doi: 10.1016/j.clnu.2024.06.009. Available at: ScienceDirect
Nunes CL, Casanova N, Francisco R, et al. Systematic review and meta-analysis of protein intake
to support muscle mass and function in healthy adults. J Cachexia Sarcopenia Muscle. 2022;13(2):795
to 809. doi: 10.1002/jcsm.12922. Available at: PMC
Morton RW, Murphy KT, McKellar SR, et al. A systematic review, meta-analysis and meta-regression
of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in
healthy adults. Br J Sports Med. 2018;52(6):376 to 384. doi: 10.1136/bjsports-2017 to 097608.
Phillips SM, Chevalier S, Leidy HJ. Protein "requirements" beyond the RDA: implications for
optimizing health. Appl Physiol Nutr Metab. 2016;41(5):565 to 572. doi: 10.1139/apnm-2015 to 0550.
Helms ER, Zinn C, Rowlands DS, Brown SR. A systematic review of dietary protein during caloric
restriction in resistance trained lean athletes: a case for higher intakes. Int J Sport Nutr Exerc
Metab. 2014;24(2):127 to 138. doi: 10.1123/ijsnem.2013 to 0054. Available at: PubMed
Pasiakos SM, Cao JJ, Margolis LM, et al. Effects of high-protein diets on fat-free mass and
muscle protein synthesis following weight loss: a randomized controlled trial. FASEB J.
2013;27(9):3837 to 3847. doi: 10.1096/fj.13 to
230227.
Yamada Y, Yoshida T, Yokoyama K, et al. Dose-response relationship between protein intake and
muscle mass increase: a systematic review and meta-analysis of randomized controlled trials. Nutr
Rev. 2021;79(1):66 to 75. doi: 10.1093/nutrit/nuaa104. Available at: Oxford Academic
Papatriantafyllou E, Efthymiou D, Zoumbaneas E, Popescu CA, Vassilopoulou E. Sleep Deprivation:
Effects on Weight Loss and Weight Loss Maintenance. Nutrients. 2022;14(8):1549. doi: 10.3390/nu14081549. Available at: PMC
Xiao Q, Chaput JP, Olds T, et al. Insufficient sleep predicts poor weight loss maintenance after
1 year. Sleep. 2023;46(5):zsac295. doi: 10.1093/sleep/zsac295. Available at: Oxford Academic
Al Khatib HK, Harding SV, Darzi J, Pot GK. The effects of partial sleep deprivation on energy
balance: a systematic review and meta-analysis. Eur J Clin Nutr. 2017;71(5):614 to 624. doi: 10.1038/ejcn.2016.201.
Nedeltcheva AV, Kilkus JM, Imperial J, Schoeller DA, Penev PD. Insufficient sleep undermines
dietary efforts to reduce adiposity. Ann Intern Med. 2010;153(7):435 to 441. doi: 10.7326/0003 to 4819-153 to 7-201010050 to 00006. Available
at: PubMed
Spaeth AM, Dinges DF, Goel N. Effects of Experimental Sleep Restriction on Weight Gain, Caloric
Intake, and Meal Timing in Healthy Adults. Sleep. 2013;36(7):981 to 990. doi: 10.5665/sleep.2792.
St-Onge MP. Sleep-obesity relation: underlying mechanisms and consequences for treatment.
Obes Rev. 2017;18 Suppl 1:34 to 39. doi: 10.1111/obr.12499.
Patel SR, Hayes AL, Blackwell T, et al. The association between sleep patterns and obesity in
older adults. Int J Obes (Lond). 2014;38(9):1159 to 1164. doi: 10.1038/ijo.2014.13.
Covassin N, Singh P, McCrady-Spitzer SK, et al. Effects of Experimental Sleep Restriction on
Energy Intake, Energy Expenditure, and Visceral Obesity. J Am Coll Cardiol. 2022;79(13):1254 to 1265.
doi: 10.1016/j.jacc.2022.01.038.
Mason AE, Hecht FM, Davis SK, et al. Obesity and sleep disorders: A bidirectional relationship.
Nutr Metab Cardiovasc Dis. 2025;35(3):103881. doi: 10.1016/j.numecd.2025.103881. Available at: ScienceDirect
Thornton SN. Increased Hydration Can Be Associated with Weight Loss. Front Nutr.
2016;3:18. doi: 10.3389/fnut.2016.00018. Available at: Frontiers
Dennis EA, Dengo AL, Comber DL, et al. Water consumption increases weight loss during a
hypocaloric diet intervention in middle-aged and older adults. Obesity (Silver Spring).
2010;18(2):300 to 307. doi: 10.1038/oby.2009.235.
Vij VA, Joshi AS. Effect of excessive water intake on body weight, body mass index, body fat,
and appetite of overweight female participants. J Nat Sci Biol Med. 2014;5(2):340 to 344. doi: 10.4103/0976 to 9668.136180. Available at: PMC
Stookey JD, Constant F, Popkin BM, Gardner CD. Drinking water is associated with weight loss in
overweight dieting women independent of diet and activity. Obesity (Silver Spring). 2008;16(11):2481
to 2488. doi: 10.1038/oby.2008.409.
Boschmann M, Steiniger J, Hille U, et al. Water-induced thermogenesis. J Clin Endocrinol
Metab. 2003;88(12):6015 to 6019. doi: 10.1210/jc.2003 to
030780.
Muckelbauer R, Sarganas G, Grüneis A, Müller-Nordhorn J. Association between water consumption
and body weight outcomes: a systematic review. Am J Clin Nutr. 2013;98(2):282 to 299. doi: 10.3945/ajcn.112.055061.
Corney RA, Sunderland C, James LJ. Immediate pre-meal water ingestion decreases voluntary food
intake in lean young males. Eur J Nutr. 2016;55(2):815 to 819. doi: 10.1007/s00394 to 015-0903 to 4.
Daniels MC, Popkin BM. Impact of water intake on energy intake and weight status: a systematic
review. Nutr Rev. 2010;68(9):505 to 521. doi: 10.1111/j.1753 to 4887.2010.00311.x.
Burke LE, Wang J, Sevick MA. Self-monitoring in weight loss: a systematic review of the
literature. J Am Diet Assoc. 2011;111(1):92 to 102. doi: 10.1016/j.jada.2010.10.008. Available at: PMC
Lutes LD, Dinatale E, Goodrich DE, et al. The Effect of Adherence to Dietary Tracking on Weight
Loss: Using HLM to Model Weight Loss over Time. J Diabetes Res. 2017;2017:6951495. doi: 10.1155/2017/6951495. Available at: PMC
Turner-McGrievy GM, Dunn CG, Wilcox S, et al. Defining adherence to mobile dietary
self-monitoring and assessing tracking over time: tracking at least two eating occasions per day is best
marker of adherence within two different mobile health randomized weight loss interventions. J Acad Nutr
Diet. 2019;119(9):1516 to 1524. doi: 10.1016/j.jand.2019.03.012. Available at: PMC
Chin SO, Keum C, Woo J, et al. Successful weight reduction and maintenance by using a smartphone
application in those with overweight and obesity. Sci Rep. 2016;6:34563. doi: 10.1038/srep34563.
Patel ML, Hopkins CM, Brooks TL, Bennett GG. Comparing Self-Monitoring Strategies for Weight
Loss in a Smartphone App: Randomized Controlled Trial. JMIR Mhealth Uhealth. 2019;7(2):e12209. doi:
10.2196/12209.
Helsel DL, Jakicic JM, Otto AD. Comparison of techniques for self-monitoring eating and exercise
behaviors on weight loss in a correspondence-based intervention. J Am Diet Assoc. 2007;107(10):1807
to 1810. doi: 10.1016/j.jada.2007.07.014.
Lemstra M, Bird Y, Nwankwo C, Rogers M, Moraros J. Weight loss intervention adherence and
factors promoting adherence: a meta-analysis. Patient Prefer Adherence. 2016;10:1547 to 1559. doi: 10.2147/PPA.S103649.
Berry R, Kassavou A, Sutton S. Does self-monitoring diet and physical activity behaviors using
digital technology support adults with obesity or overweight to lose weight? Obes Rev.
2021;22(10):e13306. doi: 10.1111/obr.13306.
Available at: Wiley
Carter MC, Burley VJ, Nykjaer C, Cade JE. Adherence to a smartphone application for weight loss
compared to website and paper diary: pilot randomized controlled trial. J Med Internet Res.
2013;15(4):e32. doi: 10.2196/jmir.2283.
Wang J, Sereika SM, Chasens ER, Ewing LJ, Matthews JT, Burke LE. Effect of adherence to
self-monitoring of diet and physical activity on weight loss in a technology-supported behavioral
intervention. Patient Prefer Adherence. 2012;6:221 to 226. doi: 10.2147/PPA.S28889.
Raber M, Liao Y, Rara A, et al. A systematic review of the use of dietary self-monitoring in
behavioural weight loss interventions: delivery, intensity and effectiveness. Public Health Nutr.
2021;24(11):3234 to 3248. doi: 10.1017/S1368980021002755. Available at: PMC
Not medical advice. Consult your doctor before starting any diet or exercise program. Use at your own risk.